21/F / Short case / IgA Nephropathy
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box is welcome."
Chief compliants:
Absent Menstrual cycle 6 months back.
History of present illness :
Patient was apparently asymptomatic 6 months back, then she developed absent Menstrual cycles not associated with any pain abdomen and vomtings and then she went to the gynecology OPD and on routine evaluation , the ultrasound abdomen showed altered renal echotexture and Urine analysis showed Proteinuria and she was referred to general medicine department for further work up.
No history of any rash over the malar areas, ulcers in the mouth and pain in the joints.
No history of any hematuria , throat pain, skin rashes.
No history of fever ,pain abdomen , cold etc.
No history of any pedal edema , shortness of breath and decreased urine output
No history of any loss of appetite, dryness of skin and vomtings .
Past history:
No history of similar complaints in the past.
History of seizures at around 2 years of age.
GENERAL EXAMINATION:
No pallor ,icterus,clubbing,cyanosis,lymphadenopathy.
Pedal edema.
SYSTEMIC EXAMINATION:
BP: 100/80
PR: 70BPM
CVS:S1S2+
RS; BAE+
P/A: SOFT,NON TENDER
Clinical images :




Investigations:
LFT -
TB -0.7
DB - 0.12
AST - 10
ALT - 08
ALP - 238
TP - 6.2
ALB - 4.19
RFT
UREA - 43
CREATININE - 3.7
URIC ACID - 7.8
Ca + - 9.6
Phosphate - 3.7
Na - 145
K+ - 4.1
Cl- 103
CUE -
ALBUMIN - 3+
RBC - 1-2
Crystals - 2+
CASTS - NIL
PUS CELLS - NIL
CBP -
HB - 9.8
TLC - 8,600
PCV - 29.4
RBC - 3.51 MILLION
PLTS - 1.66 LAKHS
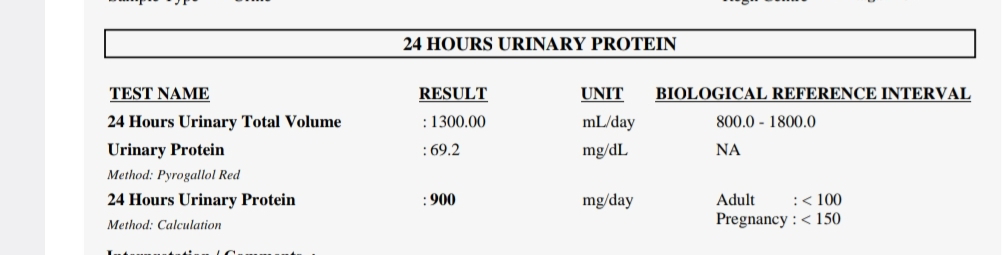
24 hour urinary protein was 900mg/ day.
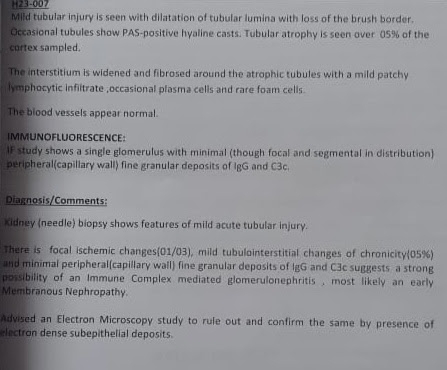
Renal biopsy:
Electron microscopy:



Treatment:
1) Tab Mycophenolate mofetil 360mg /PO/TID.
2) Tab Minipress XL /PO/OD
3) Tab Bisoprolol 2.5mg /PO/OD .
Critical appraisal:
https://pubmed.ncbi.nlm.nih.gov/36745456/
P -The role of mycophenolate mofetil (MMF) in management of immunoglobulin A nephropathy (IgAN)
I-total of 170 participants were randomized in a 1:1 ratio to receive MMF (initially, 1.5 g/d for 12 months, maintained at 0.75-1.0 g for at least 6 months) plus SC or SC alone.
C- During a 3-month run-in period, 238 patients received optimized supportive care (SC), including losartan
O-This study found that addition of MMF to SC compared with SC alone significantly reduced risk of disease progression among patients with progressive IgAN.


Comments
Post a Comment