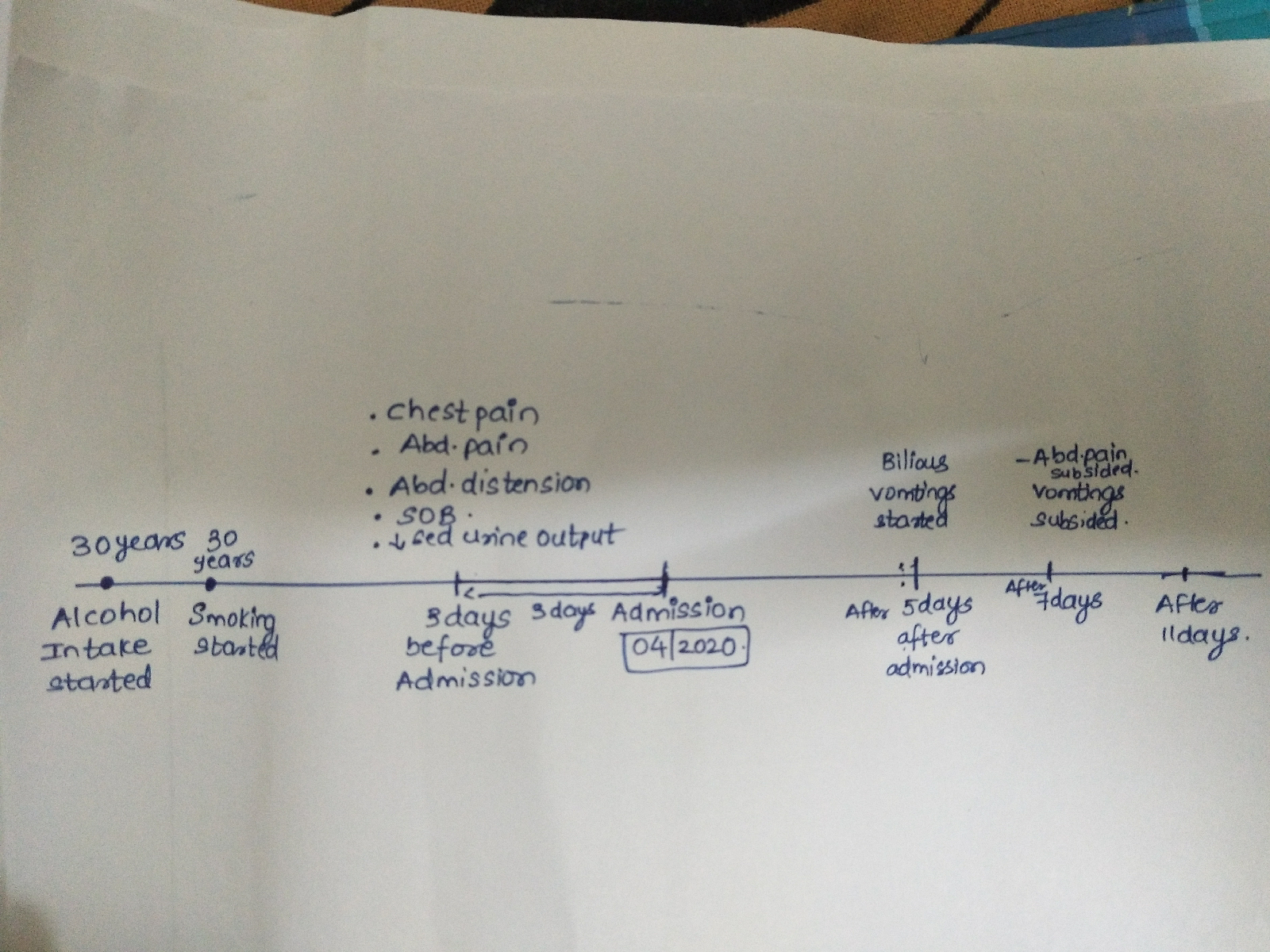
60 yr male CKD on MHD
Past history : k/c/o DM since 10years and on Medication ( given by Government ) K/C/O HTN since 7 years and on medication. Personal history : PERSONAL HISTORY: Mixed diet, Appetite normal, alcoholic(30ml/day) and Smoking 36beedis per day. No other addictions. GENERAL EXAMINATION: Patient was consious, coherent, cooperative;oriented to time,place,person. Pallor present No icterus, clubbing, cynosis, lypmhadenopathy. Bilateral pedal edema present. Investigations: Treatment: 1) Inj. Lasix 40mg /IV /BD. 2)Tab.clinidipine 10 mg /PO/ OD. 3) inj. Human actrapid insulin /SC. 4) tab. Nodosis 500mg PO/TID . 5) Tab. Shelcal CT 500mg/OD 6) Tab. Alfa D3/ PO/OD. 7) Tab. Orofer XT PO/OD. 8) Inj Ceftriaxone 1gm IV/BD. 9) Inj.Erythropoietin 4000IU /S...